Tennis elbow is probably the foremost injury that comes to mind when we think of upper-limb tennis injuries. Here at PhysioMotion we tend to see a lot of it in June/July, due to what we call “The Wimbledon Effect”.
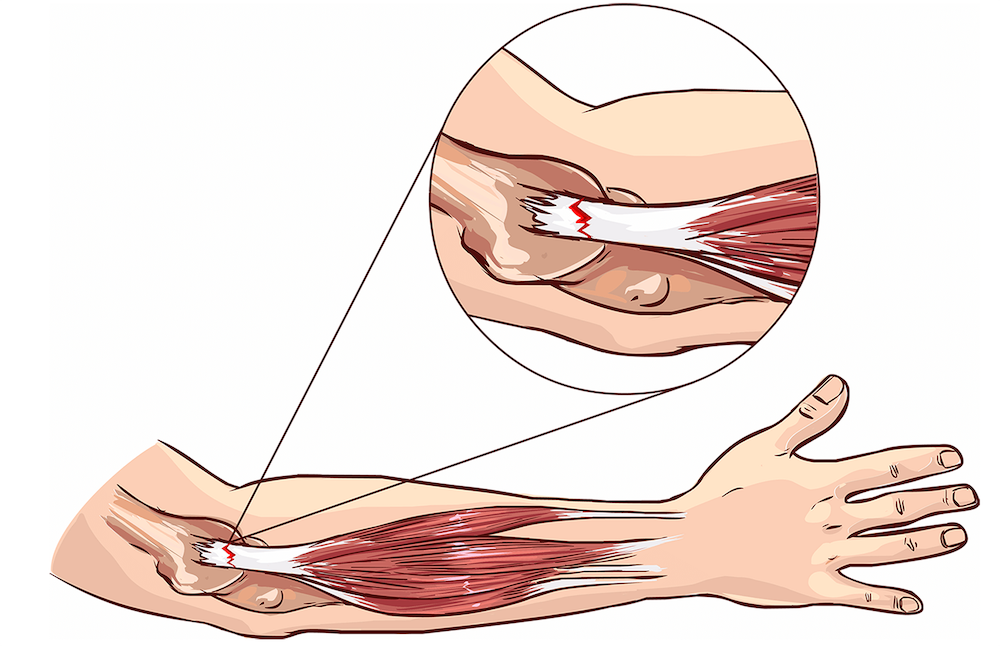
Tennis elbow (also known as lateral epicondylitis) is primarily the overuse of a muscle called extensor carpi radialis brevis (ECRB). This muscle starts at the outside of your elbow (the lateral epicondyle) and passes over your wrist and middle finger. It enables you to lift your wrist and middle finger backward.
If you have tennis elbow it will be painful to touch around the outside of elbow, and you’ll feel pain when you resist the extension (lifting back) of your wrist and middle finger. Research shows that overuse of your ECRB causes thickening in the connective tissues in an unstructured manner and irritates the surrounding nerves, rather than causing inflammation as was previously thought (De Smelt et al., 2007). Depending on the duration of symptoms, it reduces strength in the forearm muscles that pull your wrist back and assist with gripping.
Tennis elbow is far more common in recreational tennis players than with elite players. One reason for this is the quantity of time they spend playing tennis.
Recreational players suddenly increase their playing during the summer months after having played little or no tennis during the winter period. This is the equivalent to deciding to go to the gym again after 3 months non-activity and attempting to bench press 100kg 3 days in a row. Your muscles are going to be sore and you’re possibly going to cause a strain injury as they aren’t used to this level of training or being used for long periods on sequential days.
Differences in stroke technique can contribute too, as the ECRB muscle is used in all tennis strokes. If you have a poor technique it can lead to greater activity of the wrist extensors (Morris et al.,1989).This is particularly evident when playing a one-handed backhand, as with a two-handed stroke the non-dominant arm absorbs more energy and changes the mechanics of the swing (Giangarra et al, 1993).
Research has shown that the optimum wrist position is to maintain it extended to about 23 degrees from neutral alignment, with the wrist moving further into extension at impact. This is demonstrated in elite players, and their ability to reduce impact transmission from the racquet to the wrist and elbow (De Smedt et al., 2007) reducing the likelihood of tennis elbow.


Novice players maintain their wrist in a flexed position during backhand stroke, this results in overloading their wrist extensor muscles throughout the stroke, which can contribute to tennis elbow (Blackwell and Cole, 1994). They also demonstrate this flexed position during ball impact and early follow-through. Therefore when teaching novice players to hold their racquet correctly, they’re told to hold it like they’re using a hammer.
Factors that have been shown not to contribute to tennis elbow are string vibration (therefore dampers showed no significant differences in discomfort ratings) and tennis racquet grip size that showed no alteration in forearm muscle firing patterns if the racquet was over or under the recommended grip size of 6.35mm.
Our treatments for tennis elbow differ depending on how long you’ve had it and whether or not it’s a chronic problem. For acute true tennis elbow, we normally treat with stretching, acupuncture in the first 2 to 8 weeks, eccentric loading of the ECRB, and strengthening. We would also observe your stroke technique and correct any movement patterns around the shoulder, elbow and wrist that could cause or aggravate tennis elbow.
For chronic tennis elbow, once we have exhausted conservative management you may require microtenotomy surgery to the ECRB. This has shown good results in reducing pain and increasing function in the short and long term (Tasto et al., 2005), or surgery to release the extensor muscle’s tendons at the origin.
Tennis elbow symptoms can also arise due to nerve irritation of the posterior interosseous nerve that supplies signals to the ECRB muscle in your forearm. Although this can result in symptoms similar to tennis elbow, it is actually referred pain from the neck into the arm/s.
With referred pain that is coming from the neck or an irritated nerve supplying ECRB (which is not always actually tennis elbow as described above), we will mobilise the facet joints in the neck and/or use nerve glide exercises. We’ll also look at movement patterns that could be contributing to reduced nerve mobility, and stress factors that could be causing increased muscle tension.
When looking at tennis elbow, we first have to identify if it is true tennis elbow, and if so what factors in your game could be contributing to overuse of your ECRB. This will ensure that we effectively treat your symptoms and reduce the risk of them returning.
Morris M, Jobe FW, Perry J, et al. Electromyographic analysis of elbow function in tennis players. Am J Sports Med 1989;17:241-7.
De Smedt T, Jong A, Van Leemput W, Lieven D, Van Glabbeek F. Lateral epicondylitis in tennis: update on aetiology, biomechanics and treatment. British Journal of Sports Medicine 2007; 41:816-819.
Giangarra CE, Conroy B, Jobe FW, et al. Electromyographic and cinematographic analysis of elbow function in tennis playerss using single- and double-handed backhand strokes. Am J Sports Med 1993;21:394-9.
Blackwell JR, Cole KJ. Wrist kinematics differ in expert and novice tennis players performing the backhand stroke: implications for tennis elbow. J Biomech 1994;27:509-16.
Tasto JP, Cummings J, Medlock V, et al. Microtenotomy using a radiofrequency probe to treat lateral epicondylitis. Arthroscopy 2005;21:851-60.